
How I helped people get easy access to their healthcare records and designed waste out of the system

posted 10th January 2022
Service Design Lead, Discovery, May to December 2021
THE CHALLENGE
The Council, working in partnership with the NHS, wanted to improve residents’ access to their health records, ideally through the NHS App. This wasn’t just a digital delivery challenge. For the service to be viable, it had to demonstrate measurable public health benefits while also delivering efficiency gains across a stretched NHS system. I asked two questions:
- How could easy access and clear signposting to services improve individual health outcomes?
- How could the same solution reduce systemic waste, by helping people navigate care more effectively?
THE SOLUTION
Collaborating with stakeholders across clinical, administrative, and policy teams, I led the design and validation of a new service proposition.
I designed and tested future-state journeys and service blueprints, grounded in real user needs and system constraints.
The journeys helped clarify how smarter access to health services could lead to earlier interventions, better patient self-management and reduced pressure on frontline services.
IMPACT
The proposed journeys and service models were:
- Desirable – welcomed by patients and carers
- Viable – supported by NHS teams and leadership
- Feasible – aligned with existing tools, including the NHS App
The Governance Board approved further funding for design and delivery, signalling both confidence in the solution and a wider shift in mindset toward patient empowerment.
Approach (Discovery)
I took a systemic, human-centred approach from the start.
It had to work for residents and it also had to make sense for the many moving parts inside the health system, from GPs to specialists to digital teams. That meant working across boundaries, balancing different pressures and always coming back to what would create the most value for all people with the least friction.
I worked closely with a delivery lead, clinical lead, technical architect, analyst and comms specialist to bridge perspectives.
I regularly ran workshops with frontline teams, spoke with patient representatives and tested early ideas with real users. I worked with the team and checked each insight against real-world constraints: clinical policy, existing tech, operational workflows.
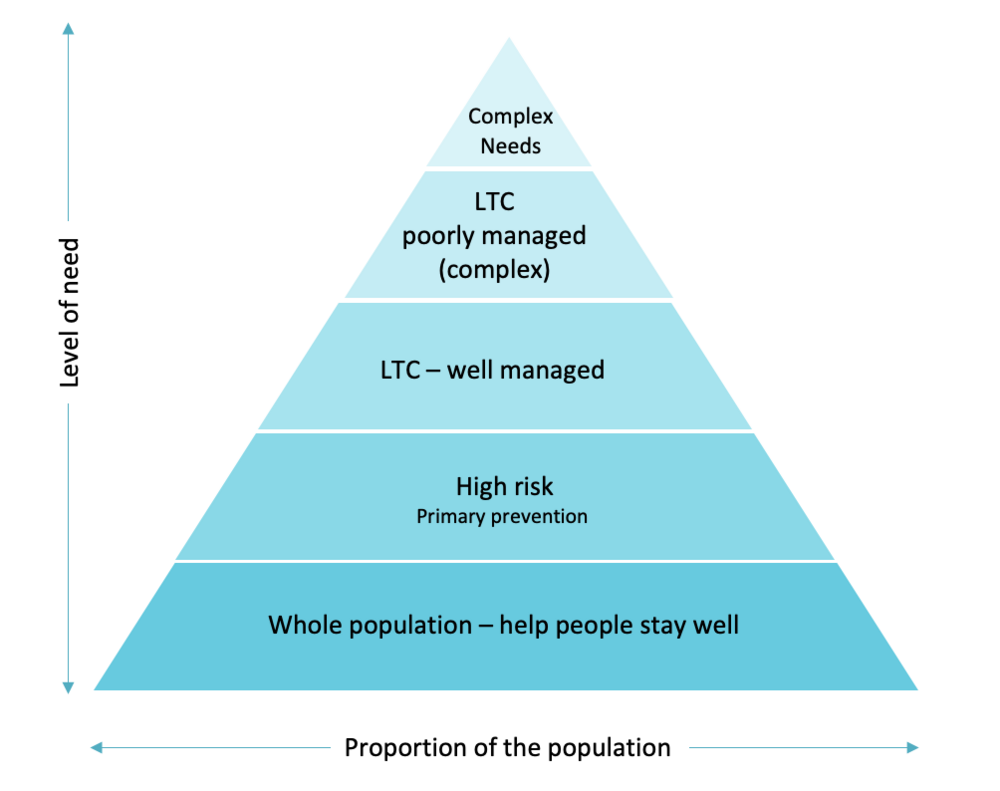
The health landscape & areas of focus
I needed to understand the healthcare landscape in more detail. The health needs pyramid below helped with this objective. I used the health needs pyramid to inform priorities and focus.
Health needs vary widely across the population. Roughly 70% of residents are mostly healthy and use the system occasionally. The remaining 30% live with long-term conditions—and account for most NHS spending.
I developed two working hypotheses with the governance board:
- If we support the healthy majority early, we can prevent more complex issues later.
- If we give people with long-term conditions more control and better tools, they’ll manage their health better and avoid crisis care.
This lens helped us frame design decisions to serve the biggest number of people and free up resources where they’re needed most.
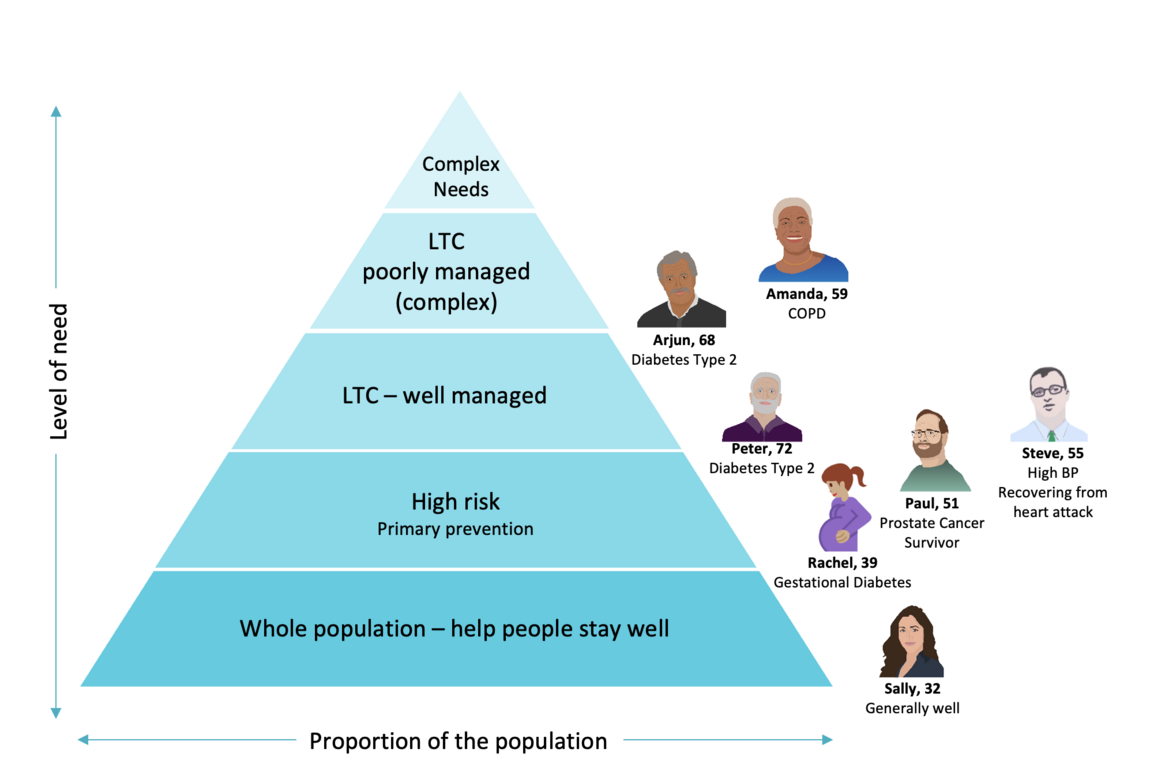
Personas and their As-Is journeys
To ensure the future patient portal met the population needs as a whole, I developed a set of personas to represent the broadest spectrum of the population.
To keep the service grounded in reality, I developed a set of personas to represent the population and their health goals:
- Healthy and independent
- Living with ongoing conditions
- Going through cancer treatment
- Managing a high-risk pregnancy
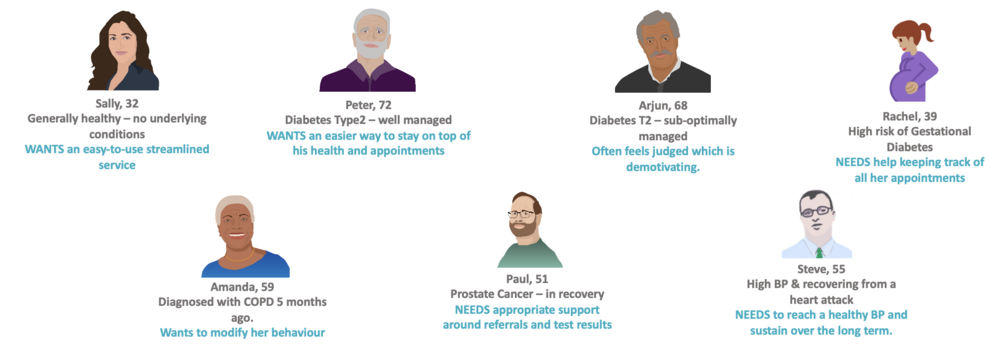
Each persona was mapped against the health pyramid and real journeys: what they do now, what gets in their way, and what better might look like.
Across all types, the frustrations were familiar:
- Not knowing what services exist
- Feeling stuck chasing referrals
- No clear picture of what’s next
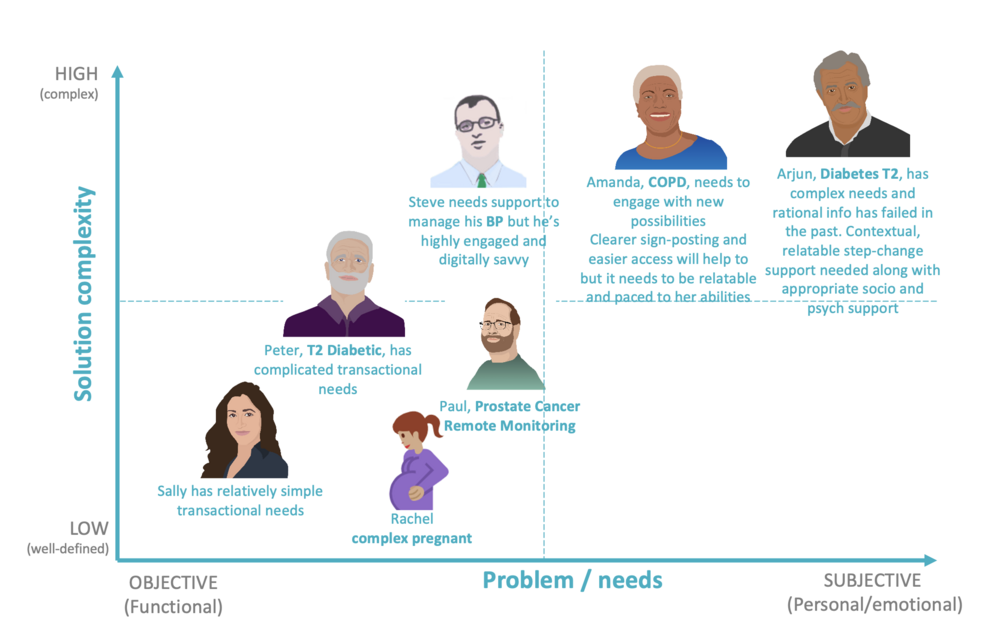
Health needs fall on a spectrum.
Some are simple and task-based. Others are emotional, long-term or tied to life circumstances.
I tested digital solutions across both ends of that spectrum.
For simpler, transactional needs, I tested features like:
- Easy access to records and care plans
- Clear referral timelines
- Self-service appointment booking
These were especially valued by digitally confident users and by GPs tired of handling chase calls.
For more complex needs, I explored hybrid solutions:
- Reminders and explanations tailored to the individual
- Access to community groups or step-by-step guidance
- Personalised tools to support behaviour change over time
Digital helped here, but it wasn’t the whole answer. What mattered was how these tools connected to existing care, rather than replacing it.
Digital exclusion is a health issue.
People at the base of the health pyramid are generally healthy and usually online. Those with more complex needs are often less digitally confident, or prefer face-to-face care. Around 20% of the population is digitally excluded and up to 35% prefer not to use digital channels, particularly older residents.
The new digital offer was designed as an addition to, not a replacement of, existing health services giving people more options, not fewer so that no one got left behind.
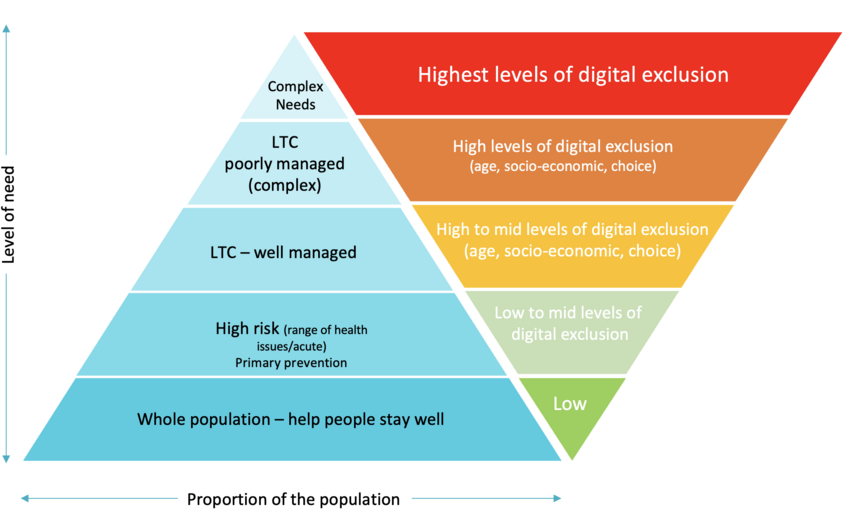
There is a strong correlation between complex health needs and digital exclusion. This is because older people are more likely to have more complex health needs and live with digital exclusion characteristics.
If a person has one or more of the following characteristics they are at risk of digital exclusion:
- Age, 65+
- Living alone
- Registered disability, especially sensory impairment e.g. blind or deaf
- English not as a first language
- Universal credit claimant
- Homeless / temporary accommodation
- Fleeing from domestic abuse
- Registered carer
- Poor mental health
The more of these characteristics they have the more likely they are to be digitally excluded.
The new proposition
The Patient Portal, ideally embedded within the NHS App, will give people access to their personal health records so they can learn about their health, choose services and treatment options that work best for them and co-manage personalised healthcare in the longer-term.
This proposition puts patients in the driver's seat and shifts the relationship with doctors from do to towards do with with expected better health outcomes in the long run.
The new digital offer was designed as an addition to, not a replacement of, existing health services giving people more options, not fewer, so that no one got left behind.
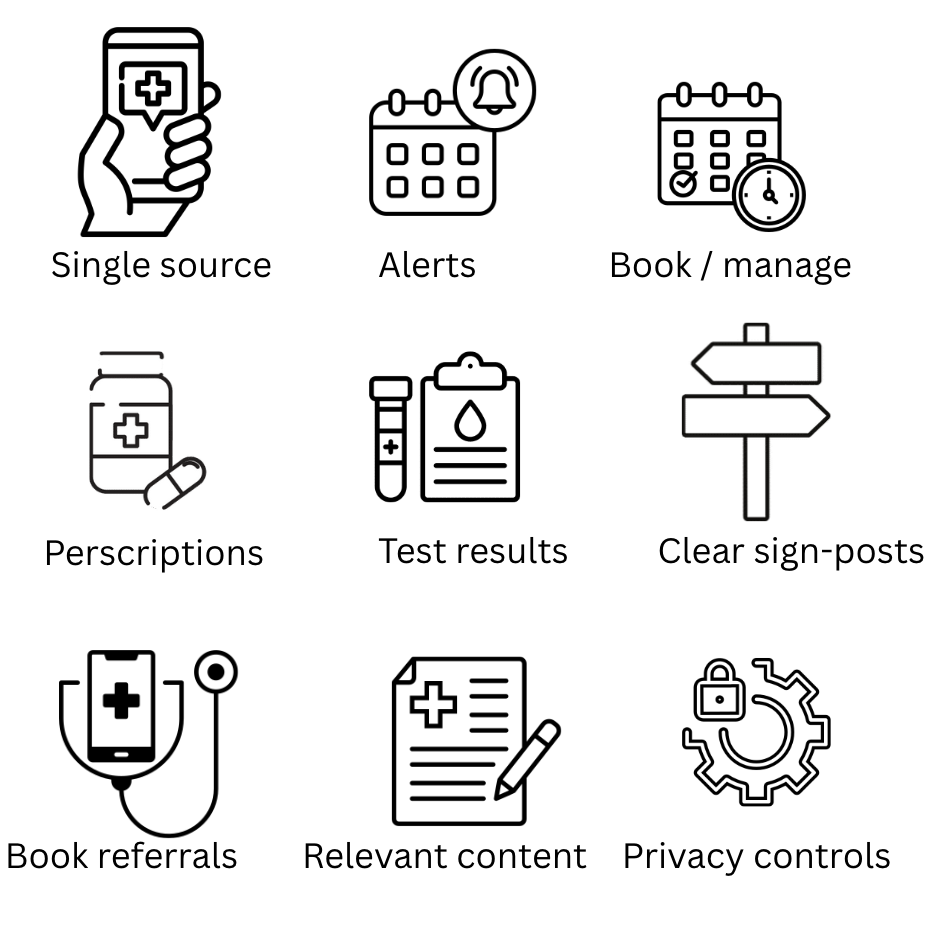
Below are the proposed features, helping to move from dispersed data to a single integrated touchpoints, better sign-posting and more agency for people and patients. .

The service enables early and more often engagement with healthcare through digital channels, which are cheaper over the longer-term. By promoting health literacy and preventative care we can nudge behaviours that keep people healthier for long. When she does need support the Patient Portal can sign-post the most appropriate (and cost effective) service.
- Hook her in early, so she is engaged if/when circumstances change
- Single point of digital access to health records through life-time of changing health needs, e.g. pregnant
- More choice – give her digital (efficiencies) as it suits her lifestyle
- Sign-post health services that align with needs, rather than default to GP (cost effective allocation of NHS resources)
- Less missed appointments (big cost saving for NHS)
This improves the service for those living with long-term conditions like diabetes. If the person is already managing their condition well, it may not necessarily improve their health, but it can help them to be more independent, incur less cognitive overload and therefore be healthier for longer.
- Digital records / single access point
- Schedule / alerts meds and appointments
- Book / manage appointments
- Monitor and track progress
- Links to contacts / diabetic team
- Additional safety net if circumstances change (Jill gets sick/dies? They move house?)

Tested & validated benefits across representative users
The proposed future-state journeys we tested showed how the proposed service could let people:
- Access the medical records they needed, in a language and format that made sense the them
- Book and manage their own appointments
- Understand care plans and referral steps
- Learn more about their condition and what to expect
Benefits for users:
- Independent and healthy poeple can self-manage and avoid unnecessary calls
- Those managing their long-term conditions well gain confidence to take more control
- Those dealing with cancer recover with better support and fewer surprises
- Those struggling to stick to his plan get the nudges and tools they needs to stay on track
Benefits for the system:
- Fewer missed appointments (a major cost)
- Fewer inappropriate GP visits (a major strain on primary care)
- Less pressure on admin staff
- Better use of existing tools, starting with the NHS App
Design challenges & how I tacked them
Finding shared opportunities in a fragmented system
- Health journeys vary widely so I needed to understand patterns.
- What worked: Mapping real journeys across diverse users helped me and the team find pivot points, where small changes could unlock bigger gains.
Balancing user needs with NHS capacity
- Some patient expectations couldn’t be met, like guaranteed face-to-face access.
- What worked: Instead of “what people want", I focused on why they wanted it. That helped us understand user bias and their blind spots and led to focusing on better sign-posting, improved communication and nudges and a more realistic service designs.
Bridging the gaps with capability & culture
- Healthcare records were traditionally owned by doctors (usually GPs), created by medical teams, for other medical teams
- What worked: Uncovered what really mattered to people, what they wanted to see and understand and pin-pointed the use cases where patients needed handholding to understand to make better decisions. This helped to understand the spectrum of challenges and quantity risk and suggest alternative journeys for high-risk cases.
The outcome
The proposal gave leaders a clear path forward and was approved for further funding. It gave patients a stronger voice and illustrated that better access isn’t just about convenience, it’s about making the system work for everyone.